Stay ahead of the curve as a political insider with deep policy analysis, daily briefings and policy-shaping tools.
Request a DemoQ&A: Health committee chair Sen. Charbonneau talks health care costs, child care and upcoming session

Sen. Ed Charbonneau, R-Valparaiso, speaks with Sen. Justin Busch, R-Fort Wayne, on the Senate floor on April 25, 2023. (Credit: Mark Curry)

This interview is part of a series of Q&As with committee chairs ahead of the 2024 legislative session to discuss the legislation that could move through their committees.
Health care dominated the 2023 legislative session, from a massive increase in both mental and public health spending, to multiple bills aimed at lowering health care costs for consumers.
The upcoming 2024 legislative session certainly won’t be that.
State Affairs spoke with Sen. Ed Charbonneau, chair of the Senate Committee on Health and Provider Services, about what issues he expects to see in his committee during the short legislative session, including more legislation targeting health care pricing. He also talked about a bill he plans to file that aims to increase child care access.
This conversation has been edited for clarity, brevity and length.
Q. What issues do you expect to focus on in your committee this upcoming legislative session?
A. We’re in a short session. Leadership is saying this is going to be fast — in and out, no big controversial issues.
We can look to summer study committees to get an idea of what may be coming down the road with certainly the [Interim Study Committee on Public Health, Behavioral Health, and Human Services] where we made recommendations on child care and psilocybin. [Some states have decriminalized psilocybin , a substance found in psychedelic mushrooms.]
The child care issue is much bigger than I realized it was before we discussed it in the summer study committee. I describe child care now as another infrastructure issue for the state of Indiana. It affects every aspect of our economy. When everybody's struggling to find people to work, this is an issue that can help allow people to go to work who might not otherwise.
The psilocybin issue, I would like to get more information on that. It certainly seems to be a promising treatment for PTSD and various other mental health issues. It's only been studied. John Hopkins University has done studies, but I would like to encourage, whether it’s Purdue or IU, to maybe do some studies.
This is a non-budget year and I am planning at this point on not having bills that have a fiscal impact. I don't know what the cut off will be, because we generally have a cut off of, whether it's $100,000 or whatever fiscal impact, that it would have to go over to [the Senate] Appropriations Committee. I just don't see in light of everything going on that they'll be welcoming many issues with a fiscal impact.
The Health Care Cost Oversight Task Force had a summer study committee report with some recommendations there, too.
I recently polled the members of the health committee to see what they had on their plate and there isn't a whole lot. So I think it could be a relatively calm session there.
One more that I'm toying around with is the 340B [drug pricing] program. It's a federal program that deals with the drug manufacturers getting their pills down to the hospitals that treat a lot of Medicaid patients, uninsured patients, such as Methodist Hospital up in Gary. That was the original intent, but I would like to get some more information on that.
Q. Can you explain what the 340B program is?
A.340B is the federal law that provides for drug manufacturers to sell mainly in underserved areas [at a] dramatically reduced price. The intent is that [hospitals] would be able to then prescribe much cheaper than they would be able to without the program. It just seems like the original legislation was horribly drafted at the federal level.
The intent was to provide drugs to those that can't afford them, and if that's the case, you wonder why we're getting so many folks that are turned over to collection agencies. The hospitals are also supposed to use that money that they're saving to do the kinds of things not for-profits should do, and it’s just not being done.
I'm sure the hospitals, maybe the [Eli] Lily’s of the world, are going to say, ‘Stay out of it. Don't make changes. This is a federal program. We don't want a mishmash of 50 different bills or requirements from 50 different states.’ I'm not doing that; I just want information.
Q. Is the concern that the hospitals are pocketing the savings associated with this program, instead of passing on the benefits?
A. Yea, and not using that money for care. The intent is they use those savings for the good of the people that need the help. I don’t think it’s being done.
Q. What are some of the other bills we might see your committee talk about this year to further reduce health care costs?
A. We're still relatively early in the bill filing process, so I don't have a good feel for what all is out there. With the short session, it will be difficult to take on big things. I think two issues to watch what happens in the future is with prior authorization and the 340B program.
Q. You mentioned the Health Care Cost Oversight Task Force issued a number of recommendations to address health care costs. Could you walk me through the recommendations?
A. A lot of these [recommendations] are just getting information. One of the things was just making it clear that the employers possess ownership and control of all the health care data relating to their covered lives, allowing an employer to conduct a third party audit of their health care claims and payment data [and] prohibiting spread pricing.
[Another recommendation] requires hospitals to give notice six months prior to the date of a merger. We're pretty much a state that has an oligopoly of some five large hospital systems.
I've said time and time again that we have not-for-profit hospitals that are operating as for-profit, when you look at, for example, up in Northwest Indiana, where there's a hospital in Hammond that closed. This is an area [with a large population of] Medicaid and uninsured folks.
Another probably significant recommendation is requiring the [pharmacy benefit managers], third party administrators, employee benefit consultants and insurance brokers to act as fiduciaries for the group plan that’s being represented.
And then [there was a recommendation to look] at Indiana physician reimbursement rates.
Q. Do you expect movement this year on Indiana physician reimbursement rates?
A. In this session, no, because we don't have the data. This is requiring that the data be reported. I would anticipate that there would probably be something during the 2025 session
Q. Last legislative session was a big health care costs session. Do you think those bills did enough, or do you think there's still more to do to reduce health care costs for Hoosiers?
A. I'll start with Senate Bill 4. That's the $225 million that we are going to be distributing to 86 of the 92 county [health departments] that signed up to be a part of this. We need to watch this; we need to watch how the money is being spent.
Bigger picture wise, this is a paradigm shift as I see it for the state of Indiana. We're actually going to focus on preventing people from getting sick as opposed to treating sick people. That's not going to happen overnight, and we have the funding for two years. So we're going to have to go back in two years and request more funding. Hopefully people feel that it's making a difference in our counties. There aren't going to be any dramatic increases in just two years, but we're going to have to show progress of some kind. That’s troubling to me.
Q. How will that law impact health care costs?
A. This ultimately should have a huge impact on costs, because we as a state [have] really good hospitals that give good service, good treatment, very expensively.
This is going to keep people out of the hospital, and it drives costs down. If you look at this long term, which we have a problem doing at times, there's no question in my mind it's going to reduce the cost of health care.
Q. What will be in the child care bill you plan to file?
A. Most of it is going to be administrative type changes — lowering the age, letting maybe high school students work in the child care area if they have supervision all the time. [We want to allow] two or three companies to come together and form a child care facility.
It is tricky because I didn't want to have anything that was going to have a fiscal impact. So we've threaded the needle, I do believe, and these will make a difference.
Q. What problem will those administrative changes solve in Indiana right now?
A. It will allow more spaces to be opened up. It will create the possibility of one authorization for a child care center to cover maybe three places. If they have two different Boys and Girls Clubs in two different areas up in Northwest Indiana here, they each have to go through their own process and pay for everything. This allows them to do just one to cover several different entities.
Q. Do you think that there can be a huge difference in child care access without more money?
A. I don't want to answer that one, because it’s going to take more money. Like with every other business in every other sector, the number one issue is people, employees. [We] need to pay who we have more and need to get more people to be able to work in, and be willing to work in, these child care settings.
Contact Kaitlin Lange on X @kaitlin_lange or email her at [email protected].
Facebook @stateaffairsin
Instagram @stateaffairsin
LinkedIn @stateaffairs
Read this story for free.
Create AccountRead this story for free
Create your free account or login to continue reading.
By submitting your information, you agree to the Terms of Service and acknowledge our Privacy Policy.
Latest Stories

Indiana appeals court chief judge on AI, mental health, and the state’s dwindling number of lawyers
Many Hoosiers may be familiar with their local courts or hear about the opinions of the Indiana Supreme Court, but a middle tier in the state’s judiciary system shapes justice through some 2,000 rulings a year.
The 15 judges of the Indiana Court of Appeals dole out opinions on everything from murder and fraud to civil and child welfare cases. Every Hoosier has the right to appeal a conviction or ruling, and the Court of Appeals, the second-highest court in the state, takes up each case sent its way.
Chief Judge Robert R. Altice Jr. has analyzed thousands of cases since being appointed by Gov. Mike Pence in 2015. Prior to that, he spent 15 years as an elected judge in Marion County.
Altice sat down with State Affairs for a discussion on the ins and outs of his court, how changes in technology and mental health care have impacted his work and what he sees as a major problem facing the nation’s judicial system.
This conversation has been edited for clarity, brevity and length.
Q. What sort of cases does the Court of Appeals hear?
A. We hear really everything except death penalty cases. If there’s a death penalty case, it goes straight to the [state] Supreme Court. Otherwise, we get it.
I’ve had to publish an opinion on a traffic court case. About 65% of our cases are criminal. Every, everything under the sun: murders, rapes, robberies, child molestation.
Then there are civil cases. We do medical malpractice suits, traffic accidents, you name it. Complex business litigation? Our court was involved.
Q. How does the appeals process work? There’s not a new trial, right?
A. I’ll give you an example. Let’s say you got a murder case and the defendant gets convicted and gets 65 years, which is the max for a murder conviction. Everybody in the state of Indiana has got an automatic right to appeal. Not everybody takes that right, but most criminal defendants do.
Somebody will write his brief for him. That attorney will find three issues that they think will result in a new trial if we rule in their favor. That’s really what the appellate process is: Are the errors committed at the trial court level significant enough to warrant a new trial?
And then the attorney general in the criminal cases will write a brief in opposition, then the appellant or the defendant can file a reply brief as well.
We sit and read transcripts and their briefs and do our own research and come to a decision as to whether or not there was error at the trial court level that warrants a new trial.
Q. How many of the 2,000 cases your court receives a year, how many are taken up by the Indiana Supreme Court?
A. It is rare. You start with the proposition that trial courts throughout the state are doing about 2+ million cases a year. That’s everything. We do 2,000 opinions a year. I think the Supreme Court writes about 60 opinions a year. That’s what their taking of ours.
But we’re considered an error-correcting court, whereas that’s really not their role. Their role is more jurisprudential. It’s “should we look at changing in this regard or changing precedent.”
It’s really an inverse pyramid, with the trial courts, I always say, doing the heavy lifting.
Our turnaround time is very quick. It’s about three months. Some states require oral arguments in every single case, but we don’t.
If you ask for an oral argument, we will sometimes grant that. We do a lot of oral arguments, but most of our oral arguments are traveling oral arguments. We travel all over the state and do live arguments. And we do those in front of high schools, small colleges, bigger schools.
We answer questions or ask questions like we normally would do, and then once we’re finished, then we have a question and answer session with the students.
Q. One thing we heard about at the State of the Judiciary is there’s an attorney shortage in the state, particularly in rural areas. How has that affected your work?
A. I think we’re seeing more pro se litigants, people representing themselves, and that can be difficult because we hold them to the same standard that we would hold a lawyer to. It can be really difficult for them. So in that regard, it has hurt.
We’ll go to traveling oral arguments in some rural county, and the bar association will host a lunch for us. We’ll go and there’ll be six lawyers in the room and I’ll say to somebody, “So how many people are in the bar?” And they’ll say, “Well, you’re looking at it.”
That access to justice is a really difficult thing that I think the state of Indiana is dealing with now. The Supreme Court has just set up a task force to look into how we can improve that. I believe law schools are looking at incentivizing young kids to go practice in rural areas.
It’s a real issue. I think a lot of it stems from the low bar passage rate of the last 10+ years. It’ll be interesting to see what the task force thinks.
Q. How has technology impacted the court?
A. Technology has been huge. All our work is done online now. The briefs are filed online.
The technology that we have to keep an eye on, and we’re already looking at, is artificial intelligence. What impact is that going to have on the courts, especially our courts?
You can punch a button and write an opinion. It’s probably not going to be very good, but as technology improves, it’s going to be. We’re kind of leery of that.
But at the same time, from a research standpoint, it’s been a very valuable tool. We’ve been using AI in that regard for researching for some time now, with Westlaw and Lexus as they’ve come out with those kinds of tools.
Q. There have been changes in how the world views mental health. How has that impacted the court?
A. I see it primarily in the sentencing arena. Before every defendant is sentenced by a trial court, a pre-sentence investigation is prepared on them. And so that’s where you see a lot of that because it discusses their entire background, and the number of people with mental health issues coming through has really increased greatly.
I think the pandemic had a lot to do with that as well. But again, the mental health issues are very much creeping into the system, and one of the things that we’re constantly working on trying to be aware of and trying to, to the extent we can with alternatives to incarceration, assist people.
Q. Are there any other challenges facing today’s judiciary?
A. I guess not necessarily my court, but courts in general. It appears to me that Congress is broken. They’re not passing laws.
So, what are we doing? We have to rely on the other two branches of government to kind of take up the slack, and that’s why you’re seeing tons of executive orders.
That’s not traditionally their job, and then you’re seeing the courts being called upon to determine whether or not those regulations are enforceable.
I see that as a long-term problem that we’ve got to get corrected.
Contact Rory Appleton on X at @roryehappleton or email him at [email protected].

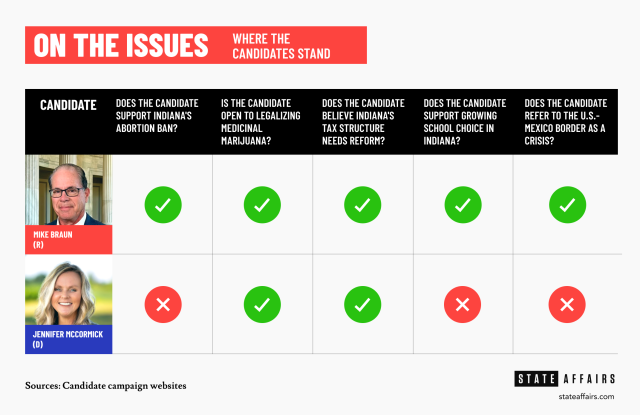
How McCormick, Braun view abortion, taxes and other key issues
A Democrat-turned-Republican and Republican-turned-Democrat will soon face off in the race to become Indiana’s next governor.
Sen. Mike Braun, who voted as a Democrat prior to 2012, captured the Republican nomination in Tuesday’s primary. Jennifer McCormick, formerly a Republican Superintendent of Public Instruction, will represent the Democrats.
Voters will decide the state’s next chief executive in November.
A State Affairs analysis of the candidates’ campaign platforms and public statements found key differences — and a few similarities — in their planned approaches to a variety of issues impacting Hoosier voters.
Here is how they match up.
Abortion
Braun: As a senator, Braun has long supported abortion restrictions.
In 2020, he called for the Supreme Court to re-examine Roe v. Wade.
In 2023, he proposed federal legislation that would have required parental notification before any unemancipated minor could seek an abortion. He said at the time: “Hoosiers put their trust in me to stand up for the unborn, and that’s what I’ve been proud to do every day in the Senate.”
He has since signaled support for the state’s abortion ban. His platform reads: “State lawmakers must work to ensure the gains we have made to protect life are secured and strengthened.”
McCormick: In a Tuesday interview with State Affairs, McCormick said her candidacy represented a referendum on reproductive rights.
“I’m going to fight to restore those rights under any authority I can, working in a bipartisan fashion, using our committees, board and our agencies. I also know, too, what everybody’s fear is: that they’re [Republicans] not going to restore those rights and will take [restrictions] further.”
From her platform: “Indiana’s Republican-led extreme abortion ban has taken away the right of women to make deeply personal decisions regarding their own health care.”
Marijuana
Braun: At a March 26 Republican primary debate, Braun suggested an openness to legalizing medicinal marijuana.
“It’s gonna hit all of us. I’m gonna listen to law enforcement — they have to put up with the brunt of it,” he said. “Medical marijuana is where I think the case is best made that maybe something needs to change. But I’ll take my cue from law enforcement there as well. … I hear a lot of input where [medical marijuana is] helpful, and I think that you need to listen and see what makes sense.”
McCormick: The Democrat’s platform also addresses medical marijuana legalization, while speculating on possible recreational use.
“We will fight for the legalization of medical marijuana as a source of state revenue established on a well-regulated marketplace and monitored by a Cannabis Task Force in order to study the issues, opportunities and potential obstructions associated with recreational marijuana legalization.”
McCormick said she would also support expunging low-level marijuana-related convictions.
Taxes
Braun: At a March 19 National Federation of Independent Business forum, Braun said the state’s property tax system “went out of whack because it couldn’t respond to inflation like we’ve never seen before.”
“The way you finance any lower taxes would be to bank on the government being run more efficiently,” he said.
His platform also calls for government spending cuts to finance lower taxes: “Reducing the size of government is the key to cutting taxes, and Mike Braun will work through every state agency to find ways to save money while delivering high-quality services to taxpayers.”
McCormick: McCormick also spoke about taxes at the March 19 forum.
“I agree with a revamp of our taxing system,” she said. “But also it’s about not just how we’re getting our revenue, it’s about our expenditures. Yes, we need to fix our gas tax. Yes, we need to look at the income tax. But here’s the thing: There are hidden taxes we’re not having a conversation about.”
Her platform also references the possibility of combining state agencies as a way to save money.
Education
Braun: In his platform, Braun supports broadening school choice and parental rights.
“As a former school board member, Mike Braun knows parents are the primary stakeholders in their children’s education and every family, regardless of income or zip code, should be able to enroll in a school of their choice and pursue a curriculum that prepares them for a career, college or the military,” the platform reads.
Braun also pledged to ensure critical race theory and discussions about gender are banned in public schools.
McCormick: Education is one of McCormick’s primary issues, according to her platform.
She calls for the elimination of statewide testing, increased early childhood reading and child care options and a minimum base salary of $60,000 for all K-12 teachers.
McCormick also addresses the state’s school choice movement.
“We will call for a pause in the expansion of school privatization efforts while requiring fiscal and academic accountability and transparency for all of Indiana schools that receive public tax dollars,” her platform reads.
U.S.-Mexico border
Braun: Braun’s television ads have touched on border security, and his platform calls for increased focus on the area.
“Joe Biden and the left have created a humanitarian and national security crisis on our southern border,” the platform reads. “As governor, Mike will continue to support and enact the America First policies that were working. Otherwise, every town will become a border town.”
McCormick: McCormick’s border-related plans are more focused on facilitating legal immigration.
“We will work with local, state and federal officials in supporting an immigrant system that creates a safe, timely, orderly and humane pathway for those seeking legal immigration while keeping our communities and those responsible for border security safe,” her platform reads.
Contact Rory Appleton on X at @roryehappleton or email him at [email protected].

Spartz, Shreve, Stutzman win Republican congressional primaries
A central Indiana congresswoman successfully fought off eight primary challengers, while crowded races for three other Republican-leaning congressional districts began to clear in Tuesday’s primary election. And in northeastern Indiana, a former congressman held on in a tight race as he seeks to return to Congress. All of the state’s nine U.S. House of Representatives …
Mike Braun wins the Indiana Republican nomination for governor
U.S. Sen. Mike Braun was declared the winner of the Republican gubernatorial nomination shortly after polls in Indiana’s Central Time Zone closed. With 98% of votes counted as of Wednesday morning, Braun had 39.6%, followed by Lt. Gov. Suzanne Crouch with 21.8%, Brad Chambers with 17.5%, Eric Doden with 11.9 %, Jamie Reitenour with 4.8% …